Substance abuse is one of the primary issues that eat up most of the families across the globe. This blog focuses on the best way you can choose an inpatient drug rehab centre for your loved ones. Rehab centres these days help greatly in defeating the addiction that you or your loved ones have and can help in bringing your life back on track again. The various factors that you need to consider while choosing an inpatient drug rehab include the cost factor and your insurance coverage. Eventually, find out facilities that give personalised care to the patients along with comprehensive inpatient treatment. Check the visitation policies and the continuum of care post the treatment as well. Lastly, the journey is gratifying if you and your family members are getting support from each other.
0 Comments

Younger adults are much difficult to put back on track from malicious substance abuse. It is because you cannot really stop them from going out or attend their college. This blog focuses on how you can select the best rehab centre for them. Whenever you are thinking of starting your research about the rehab that your younger adult needs, you need to first figure out the needs and the goals of the rehab program. You need to have a consultation done with the professionals and get the entire insight into the process of treatment. Eventually, start finding rehab options that you might feel are suitable for your needs. Also, make sure that you are considering the various other amenities available at the rehab as well. These can include outpatient or inpatient rehab, various therapies, and treatments available at the rehab, and the various specialities and amenities of the rehab. One of the main disorders that humans are dealing with includes drug addiction. This blog focuses on finding the best drug rehab and the important things you need to know about these. Drug rehab centers basically make the life of the patient free of substances and drugs. They are also extremely helpful in preventing or decreasing the frequency of the relapse after the treatment is over. The patients are dealt with round the clock and are offered an atmosphere which can help them recover and heal themselves. Though it is challenging to an extreme level to find a suitable drug addiction treatment facility but then you need to evaluate your options and then choose the one which is best needed for you and your condition. Get the professional help instantly at these drug rehabs. 
A psychological construct that involves a kind of unhealthy relationship which people share with those who are closer to them is called co-dependency. This blog focuses on the various ways codependency can be a great problem in relationships. But then you must be strong enough to recognize the signs and indication of the codependency. It makes a person feel worthless and it lowers down the self-esteem. People tend to project their image as a perfectionist and thus making themselves responsible for enduring more burden on their shoulders as compared to their partners. These people always look for validation or else may depict traits of controlling or possessive behavior. They also start giving more importance to others rather than themselves and they do it by denying their needs and existence. This is another form of abuse and must be dealt with appropriately. 
Meditation has many advantages and the primary ones being recharging the mind and body and also improving clarity and boosting concentration. In case you are already meditating, the blog shows how you can still improve it. First of all, you need to create a private place which allows you to disconnect from stress and internal worries. Using this meditation space, you can release your stress and find serenity. You can also choose a place where you get the morning sunlight. In case you have a smaller house, you need to make room by replacing a lavish sofa with comfortable chairs and using wall cabinets in place of freestanding bookshelves. In case you have a huge spacious house, you need to meditate at a place which is free of distractions. Avoid places where you are near the traffic and ensure that you are keeping your meditation space neat and clean of all the clutter. Using fragrant candles also will help enormously. 
The blog focuses on Attention Deficit Hyperactivity Disorder or ADHD is a condition which affects younger children and adults. The basic symptoms of this disorder involve a limited span of attention, not able to remain still for a long time and high levels of activity. Though these are common behaviors found in children, but, a child who has ADHD is highly inattentive and hyperactive. It can be classified into inattentive type, impulsive/hyperactive type and combined type. The treatment to this disorder is important or else it would put them at a higher risk of developing anxiety, depression and addiction. Some of the possible symptoms include low self-esteem, procrastination, mood swings, relationship issues, employment issues and so on. It is important to get a specialised treatment through a facility which caters to the unique requirements of the patients. 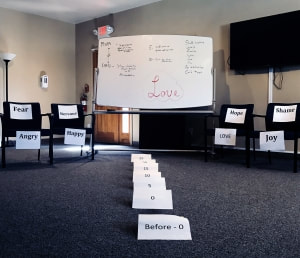 At the Claudia Black Young Adult Center, trauma is described as anything less than nurturing. This definition allows for all traumas, big or small, to be acknowledged and honored. In doing so, the client’s protective defense mechanisms such as denial, rationalization or minimization are explored and challenged so that healing can finally take place.
Types of trauma can include chronic illness, death of a loved one, physical abuse, sexual abuse, unbearable ridicule by a caregiver during childhood, or verbal and psychological abuse experienced within an intimate relationship. Trauma can also be the loss of a job promotion, a lost friendship, witnessing harm to a loved one, or unescapable harassment at school or work. In recognizing the potential lasting effects of these traumas, at the Claudia Black Young Adult Center each young adult completes a trauma timeline which allows them the opportunity to explore how trauma has affected them in the past and how it may still be impacting their present-day life. A trauma timeline begins as a pen and paper assignment of constructing a detailed history of one’s painful life experiences that left them feeling abandoned, unsafe, confused, fearful, sad, angry, shameful, guilt-ridden or stuck. Then they identify the distorted self-beliefs that are connected to the events and assess their methods for adapting, surviving, and avoiding the pain that accompanied the trauma. All of this is revealed within a small group composed of supportive peers under the careful facilitation of a skilled therapist. The sharing of these vulnerable experiences allows peers to make connections with each other resulting in shame reduction, self-compassion, self-acceptance, and self-forgiveness. While recognizing that he or she is not alone, each young adult finds the courage to face these wounds, let go of beliefs about self that are no longer serving them, and discover new empowering truths about self. The gift the trauma timeline process provides can be seen through Jessica’s experience. At the age of 20, Jessica had several previous treatment experiences and felt very defeated believing that the Claudia Black Young Adult Center would have nothing to offer her. Jessica endured a very difficult upbringing. Her parents divorced when she was quite young, which fueled great instability during Jessica’s childhood. Home was not a safe place. She found herself in the middle of her parents’ chronic battles, each vying for her undivided love and trust. Each parent pitting Jessica against the other. This only pushed her further away from both of them, and as the pain became too unbearable, Jessica coped by developing impenetrable walls, which locked in the trauma and prevented true intimacy. Her experiences of chronic instability led to an overcompensating desire for safety, which she learned early on could only come from self. This would have unintended consequences for Jessica; such as, a deep mistrust of others, unhealthy relationship patterns and the silencing of her own inner pain. Jessica made it abundantly clear that her walls were up, and she was always ready for danger. Each trauma timeline is unique; there is something very special about witnessing a client courageously taking the risk to share their pain with the group. The timeline itself is a deeply explorative and powerful exercise. However, I felt Jessica could further benefit from bringing an aspect of her timeline to life through a holistic and adaptable experiential process to provide her with more clarity and instill some hope. The beauty of experiential-based therapy is that nothing is scripted, and everything is used to foster an organic moment of truth with new insights and hope not just for the client but for each member in the group. Jessica’s work speaks to just how powerfully trusting the process can truly be. At the beginning of her timeline presentation, Jessica shared that her only goal was to learn more about her struggle to connect with others. After offering support for her willingness to share her story, and giving the group instructions around safety, confidentiality, and a general sense of what the process could look like, I asked Jessica to describe her family of origin. She described her dad as “strong, hardworking, diligent, lectures a lot” and described mom briefly as “super-psycho.” I wrote her words on the white board. Jessica shared that around age five, she learned that her own crying would “shut mom down and give mom crazy eyes.” She shared how she was told by her mom, “I never wanted you and I wish you’d never been born.” Jessica’s voice began to shake as she started to get in touch with painful emotions but quickly resorted to intellectualizing her story to avoid the pain. I invited her to slow down her words and brought her attention to the feelings she struggled to experience. For Jessica, this was the beginning of a turning point in her work. As the process transitioned toward an experiential approach, I invited Jessica to “set up” this memory so that she could visually show what her pain at age 10 looked and felt like. I covered the floor with pieces of paper with different identified feelings (e.g., pain, fear, joy, passion) and asked her at times to pick up the feelings listed to help her connect with walled-off emotions she struggled to allow herself to feel. As Jessica recalled her mom’s words of, “I wish you were never born” the group held the space for her to feel the reverberation of that pain. From the floor Jessica picked up the emotions of sadness, anger, and fear while sharing. I asked, “What do you remember feeling the most around this time in your life?” She replied, “I felt like such a burden” and quickly added, “I want to leave this room.” As she looked at the nearest door, I gave her permission to do so. Jessica froze and didn’t leave. It was clear that in that moment, she had to confront her desire to run away to avoid pain. I asked, “What do you need right now?” She tearfully said, “Love.” The feelings sign for love was still on the floor. I asked her to pick someone in the room to role-play ‘love’ and place them anywhere in the room to show how connected or disconnected to ‘love’ she currently felt. She chose a peer, and placed the peer holding the sign for ‘love’ in the corner, not facing her. Her hands tightened around the emotions she was currently holding which were sadness, anger, and fear. She then added shame, guilt, and pain. I asked, “What would ‘love’ say if it could talk to you?” She responded, “I love you, you are lovable.” I directed ‘love’ to repeat the lines, and as she did, Jessica suddenly began to honor her tears and pain. The trauma that had been frozen inside was beginning to thaw as she allowed herself to cry. Her stored up pain and anguish that existed in silent suffering was given a moment to experience the healing power of love and she knew exactly what she needed! Jessica concluded her work by dropping her carried sadness, anger, fear, shame, guilt, and pain and embraced ‘love’ with a long overdue hug. She then invited the group to share their feedback and there was a moment where she expressed gratitude to the room for all of the support during her work. After her trauma timeline, I asked Jessica to keep the piece of paper with the emotion ‘love’ as a token of her work for that day. Facing one’s pain is the start of something amazing and I hope it will encourage her to trust her needs, while acting as a reminder that she has the ability to love herself, which is an incredible source of empowerment and hope. Content source  If you haven’t already noticed, you will likely start to see some significant changes to how your food is packaged and sold.
Rolling out Obama-era policies, the Food and Drug Administration (FDA) is requiring food makers to implement a new Nutrition Facts label, which will include the following information and updates [1]:
 Resilient qualities are not only what we’re born with but also the strengths that we build through encountering life’s challenges and developing the personal and interpersonal skills to meet them. It is one of life’s paradoxes that the worst circumstances can bring the best out of us. According to the Adverse Childhood Experience (ACE) studies performed by Robert Anda (2006) and his team at Kaiser Permanente’s Health Appraisal Clinic in San Diego, we will all experience four or more serious life stressors that may be traumatizing, and according to positive psychology research, most of us will grow from them.
What Do We Mean by Resilience? Research on resilience used to view resilient qualities as residing exclusively within an individual. Today this research takes the more dynamic view of seeing resilience as an individual’s ability to mobilize supports within a social context. Wong and Wong (2012) write that “In the early days of resilience research, the focus was on ‘the invulnerable child,’ who did better than expected despite adversities and disadvantages . . . [D]evelopmental psychologists were interested in individual differences and the protective factors that contributed to the development of the invulnerable child”. Rutter, however, argues that “resilience may reside in the social context as much as within the individual” (Wong & Wong). “His concept of the ‘steeling’ effect highlights the essence of resilience — the more experience you have in overcoming adversities, the more resilient you will become” (Wong & Wong, 2012). Wong and Wong propose that certain qualities of behavioral resilience can only be developed from the actual experience of having overcome adversities (Wong & Wong, 2012). Additionally, they identify at least three prototypical patterns that resilient people appear to display, which may occur in different contexts for different individuals. These are developed as individuals meet life challenges; they are dynamic, constantly evolving qualities rather than qualities residing only within the individual. Recovery: bouncing back and returning to normal functioning Invulnerability: remaining relatively unscathed by the adversity or trauma Posttraumatic growth: bouncing back and becoming stronger (Wong & Wong, 2012, p. 588). Our Deep Need to Connect: How Early Attachment Can Be Life Enhancing or Traumatizing Our highest and most evolved system, our social engagement system, is activated through our deep urge to communicate and cooperate. From the moment of birth, our mind-body reaches out toward our primary attachment figures to establish the kind of connection that will allow us to survive and find our footing in the world. We fall back on our more primitive systems of defense — such as fight, flight, or freeze — only when we fail to find a sense of resonance and safety in this connection (Porges, 2004). The body of work that researchers Dan Siegel and Allan Schore have developed, which underlies interpersonal neurobiology, postulates that our skin does not define the boundaries of our beingness; from conception, we resonate in tune or out of tune with those around us (Schore, 1999). Through relational experiences that form and inform our sense of self and through our ability to be cared for and care about others, our capacity for empathy is formed and strengthened (Schore, 1999). Neuroception, a term coined by Stephen Porges (2004), former Director of the Brain-Body Center at the University of Illinois at Chicago, describes our innate ability to use intricate, meaning-laden, barely perceptible mind-body signals to establish bonds and communicate our needs and intentions. While many of these communications are conscious, still more occur beneath the level of our awareness in that animal-like part of us(Porges, 2004). Neuroception is a system that has evolved over time to enable humans and mammals to establish the mutually nourishing bonds that we need to survive and thrive. It is also our personal security system that assesses, in the blink of an eye, whether or not the situations that we’re encountering are safe or in some way threatening (Porges, 2004). According to Porges (2004), our neuroception tells us if we can relax and be ourselves or if and when we need to self-protect. If the signals that we’re picking up from others are cold, dismissive, or threatening, that system sets off an inner alarm that is followed by a cascade of mind-body responses honed by eons of evolution to keep us from being harmed. That mind-body system sets off equivalent alerts if we’re facing the proverbial saber-toothed tiger or saber-toothed parent, older sibling, a school bully, or spouse. We brace for harm to our person on the inside as well as on the outside. When Parents Turn Away Trauma in the home has a lasting impact. When those we rely on for our basic needs of trust, empathy, and dependency become abusive or neglectful, it constitutes a double whammy. Not only are we being hurt and confused but the very people we’d go to for solace and explanation of what’s going on are the ones causing us pain. We stand scared and braced for danger in those moments, prepared by eons of evolution, ready to flee for safety or stand and fight. If we can do neither, if escape seems impossible because we are children growing up trapped by our own size and dependency within pain engendering families, then something inside of us freezes. Just getting through, just surviving the experience becomes paramount. Relational trauma impacts all facets of the mind-body social engagement system including limbic resonance, touch, expression, gesture, sign language, and finally words. Consequently, ferreting out just what has hurt us can be a very layered process. A parent who wears a scowl all of the time, for example, and who we couldn’t reach with our attempts at connection or who begrudgingly reached for our hands and dragged us across a street or humiliated us for our small efforts share our feelings to take care of ourselves, can leave a legacy of hurt behind them. In trauma engendering interactions, “people are not able to use their interactions to regulate their physiological states in relationship . . . they are not getting anything back from the other person that can help them to remain calm and regulated. Quite the opposite. The other person’s behavior is making them go into a scared, braced-for-danger state. Their physiology is being up regulated into a fight/flight mode,” says Porges A failure to successfully engage and create a sense of safety and cooperation or to communicate needs and desires to those people we depend upon for our very survival can be experienced as traumatic. This can set the groundwork for a life long problem with self-regulation. When Children Withdraw Into Themselves For small developing children, this refusal of connection can be traumatic if it occurs consistently over time. The child can feel that their needs are somehow incompressible if the parent does not tune into him or her. Small children have little recourse when they are young and dependent. If a parent does not support a comfortable connection, if the parent or caretaker is not available for a caring co-state in which communications on both sides are met with reciprocal attempts to understand and continue to participate in a mutually satisfying feedback loop, the child may feel very alone. They may retreat into their own little world or even dissociate. After all, why continue to try when you are getting nothing back? What about the child who is disciplined not according to their own behavior but by their parent’s mood and left unable to figure out how to act to stay out of trouble? Or how about the kid in a rage-filled home who is told to sit still and listen as the parent dumps a load of pain all over them? What recourse does this child have but to flee internally? When we dissociate, we do not process experiences normally. We do not feel it, think about it, or draw meaning from it. How Early Relational Trauma Affects Our Relationships People who have been traumatized in their intimate relationships can find it difficult simply to be in comfortable connection with others. The dependency and vulnerability that is so much a part of intimacy can trigger a person who has been traumatized in their early, intimate relationships into the defensive behaviors that they relied on as children to stay safe and to feel whole rather than splintered. To heal this form of relational trauma, we need to understand what defensive strategies we used to stay safe and then shift these behaviors to be more engaged and nourishing both within our relationships and ourselves. After all, if we constantly brace for danger and rejection, then we are likely to create it. It can become a self-fulfilling prophecy. The Long-Term Impact of Parental Addiction Experiences like growing up with parental addiction and the chaos and stress that surround it pop up over and over again as primary causes of toxic stress. Anda and his team were not looking for the effects of addiction in their research however it consistently emerged as an underlying factor in ACE’s. Not only are the effects of parental addiction devastating for children, but addiction is rarely a factor by itself, it is often surrounded by a cluster of other problems such as abuse and neglect. Alcohol and drugs are often used to mask depression and anxiety in the addict but rather than make depression or anxiety better; addiction makes them worse because the depression and anxiety remain undealt with and the addiction becomes a whole, new problem of its own. And being married to an addict creates pain in the partner which undermines their ability to be a present parent, so kids lose two parents. ACEs or adverse childhood experiences tend to cluster; once a home environment is disordered, the risk of witnessing or experiencing emotional, physical, or sexual abuse actually rises dramatically (Anda, et al., 2006). During one of his lectures, Dr. Anda described why ongoing traumatic experiences such as growing up with addiction, abuse, or neglect in the home can have such tenacious effects: “For an epidemic of influenza, a hurricane, earthquake, or tornado, the worst is quickly over; treatment and recovery efforts can begin. In contrast, the chronic disaster that results from ACEs is insidious and constantly rolling out from generation to generation” (personal communication). If the effects of toxic stress are not understood so that children can receive some sort of understanding and support from home, school, and community, these children simply “vanish from view . . . and randomly reappear — as if they are new entities — in all of your service systems later in childhood, adolescence, and adulthood as clients with behavioral, learning, social, criminal, and chronic health problems” (Anda, et al., 2010). Growing up is painful; families are only human after all. We will inevitably get hurt. But we need to repair that hurt in some way, and if repair doesn’t happen at or near to the moment of the pain, it will need to happen later. When emotional pain remains split off, it becomes somehow invisible to the naked eye, and it emerges as if it a whole new problem with whole new people. But we need to embrace the challenge as adults of understanding our own childhood ACE-related pain and cleaning up its effects so that it doesn’t become the pain pump for today’s problems. The idea of growth through suffering or pain is not a new one. The systematic study of it is. Post-traumatic growth (PTG), a phrase coined by Drs. Richard Tedeschi and Lawrence Calhoun — editors of The Handbook of Post Traumatic Growth — describes the positive self-transformation that people undergo through meeting challenges head-on. It refers to a profound, life-altering response to adversity that changes us on the inside as we actively summon the kinds of qualities like fortitude, forgiveness, gratitude, and strength that enable us to not only survive tough circumstances but also thrive. Facing childhood pain and dealing with it rather than acting it out or medicating is part of post-traumatic growth and part of how we create resilience today. REFERENCES Anda, R. F., V. J. Felitti, D. W. Brown, D. Chapman, M. Dong, S. R.Schore, A.N. (1999). Affect Regulation and the Origin of the Self. Dan Siegel: The Neurological Basis of Behavior, the Mind, the Brain and Human Relationships Part 1 At the Garrison Institute’s 2011 Climate, Mind and Behavior Symposium, Dr. Dan Siegel of the … NEUROCEPTION: A Subconscious System for Detecting Threats and Safety STEPHEN W. PORGES University of Illinois at Chicago Copyright 2004 ZERO TO THREE. Reproduced with permission of the copyright holder. Schore, A.N. (1991), Early superego development: The emergence of shame and narcissistic affect regulation in the practicing period. Psychoanalysis and Contemporary Thought, 14: 187–250. — — — — — — — (1994), Affect Regulation and the Origin of the Self: The Neurobiology of Emotional Development. Mahwah Dan Siegel: The Neurological Basis of Behavior, the Mind, the Brain and Human Relationships Part 1 At the Garrison Institute’s 2011 Climate, Mind and Behavior Symposium, Dr. Dan Siegel of the …, M. (2004). Nurturing hidden resilience in troubled youth. Toronto, ON: University of Toronto Press. Wong, P. T. P. & Wong, L. C. J. (2012). A meaning-centered approach to building youth resilience. In P. T. P. Wong (Ed.), The human quest for meaning: Theories, research, and applications (2nd ed., pp. 585–617). New York, NY: Routledge. Content Source
The tray is a blank canvas in which the clients’ world is displayed through the use of miniature figures, which could be mythical protective figures, spiritual figures, family figures, animals, vegetation, fences, bridges, and addiction paraphernalia. The client leads the session, mindfully arranges the figures and then adds words to the story. The agitated lower brain is being calmed through tactile stimuli which are interpreted by the limbic system. This results in left and right brain integration, new neural pathways, greater nervous system regulation, less anxiety, and a stronger sense of safety. The very touch of the sand activates the brain in that sensations travel to the prefrontal cortex which makes sense of tactile input. Both the sand and the blue color in the box trigger neurotransmitters to calm the entire body, lowering blood pressure, slowing down pulse rate and providing a greater ability to handle threatening material. All of this lessens the flight/fight response that the client is often experiencing on an ongoing basis.
Let me tell you about Emily who was attacked while hiking, raped by three men and left in the woods. Her life fell apart. She couldn’t handle the daily functions of life let alone perform at work or engage with others socially. Using the sand tray was key to beginning her trauma work. Her hypervigilance and over-arousal state were so significant she couldn’t sit with herself or with others. She was over-aroused by the tools of EMDR and was extremely dissociative. The first session is all about creating a safe scene of what it would be like to have the sensation of calmness and safety. Safe scenes in the tray will be filled with protectors, helpers, and resources. When Emily was done, we took a picture of her sand tray, and she was to post it in her room, and also carry a picture of it wherever she was on campus. I wanted her to have this sense of safety available to her at all times. In future sessions, once she felt that safety was on board, she started to slowly bring in details of the event to the sand tray. While she cannot change the experience, with the metaphorical figures, she can create a new internal story building resilience and empowerment. By projecting onto the tray, Emily also creates enough therapeutic distance to move into a deeper emotional state where it then becomes tolerable to release stored body energy. It is here I now use the tools of somatic experiencing therapy to release the energy, weaving somatic experiencing work with sand tray. After four sessions using the sand tray, Emily no longer avoided eye contact, held her head down, or looked defeated and scared. Her body now had a stance of power. New beliefs about the event and herself emerged as she articulated “it’s over now…I can move forward….I am okay.” Given the nature of the trauma, Emily would need continued therapy, but she now has enough resources on board to move forward with more trauma work and the ability to use a wider range of mediums. As a therapist being able to use mediums such as the Sandtray with trauma survivors, I get to witness the miracles of transformation. Heidi Kaminski, MSW, LCSW is a trauma therapist at the Claudia Black Young Adult Center. While trauma-informed care is pervasive throughout the program in groups and individual sessions, clients see Ms. Kaminski specifically when they can benefit from EMDR, SE, and focused work on traumas utilizing mediums such as the Sandtray and Expressive Arts. Heidi Kaminski also has a private practice located in Peoria, Arizona. |